on line chapter 6 respiratory system

Chapter 6
Respiratory System
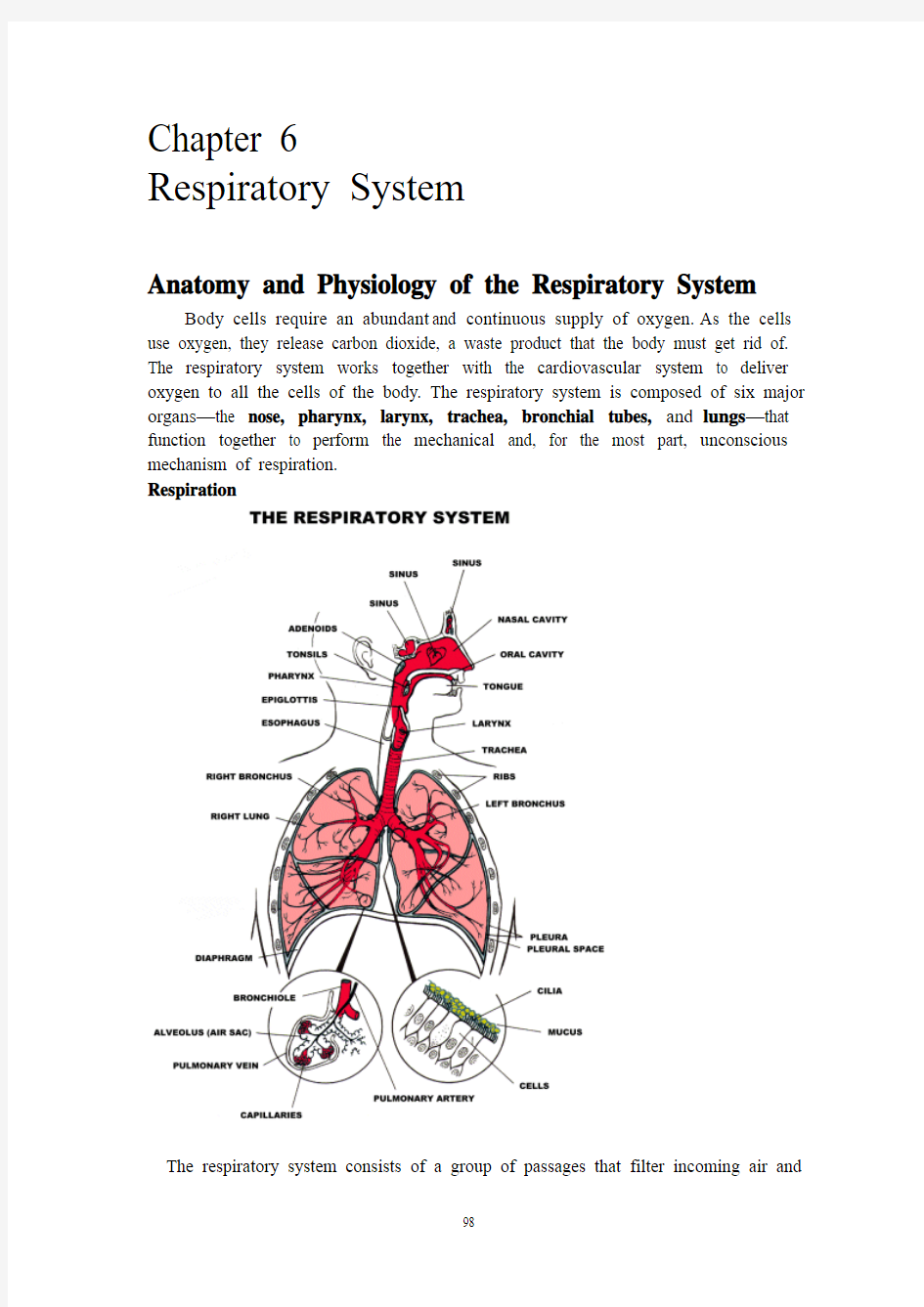
Anatomy and Physiology of the Respiratory System Body cells require an abundant and continuous supply of oxygen. As the cells use oxygen, they release carbon dioxide, a waste product that the body must get rid of. The respiratory system works together with the cardiovascular system to deliver oxygen to all the cells of the body. The respiratory system is composed of six major organs—the nose, pharynx, larynx, trachea, bronchial tubes, and lungs—that function together to perform the mechanical and, for the most part, unconscious mechanism of respiration.
Respiration
The respiratory system consists of a group of passages that filter incoming air and
transport it into the body, into the lungs and to the many microscopic air sacs where gases are exchanged. The entire process of exchanging gases between the atmosphere and body cells is called respiration. It involves at least four events:
Pulmonary ventilation: The tidelike movement of air into and out of the lungs so that the gases in the alveoli are continuously changed and refreshed. Also more simply called ventilation, or breathing.
External respiration: The gas exchange between the blood and air-filled chambers of the lungs(oxygen loading/ carbon dioxide unloading).the gases diffuse in opposite directions between the air sacs of the lungs and the bloodstream. Oxygen enters the bloodstream from the air sacs to be delivered throughout the body. Carbon dioxide leaves the blood stream and enters the air sacs to be expelled from the body during exhalation.
Transport of respiratory gases: The transport of respiratory gases between the lungs and tissue cells of the body accomplished by the cardiovascular system, using blood as the transport vehicle.
Internal respiration: Exchange of oxygen and carbon dioxide at the cellular level. At this time oxygen leaves the bloodstream and is delivered to the tissues. Oxygen is necessary for the body cells’metabolism, all the physical and chemical changes within the body that are necessary for life. The by-product of metabolism is the formation of a waste product, carbon dioxide. The carbon dioxide enters the bloodstream from the tissues and is transported back to the lungs for disposal. Internal respiration is sometimes referred to as tissue breathing since the cells within the body also must breathe fresh oxygen or, in other words, have a fresh supply of oxygen to maintain life.
Nose
Air generally passes into the respiratory tract through the external nares (nostrils), and enters the nasal cavity (divided by the nasal septum). It then flows posteriorly over three pairs of lobelike structures, the inferior, superior, and middle nasal conchae, which increase the air turbulence. As the air passes through the nasal cavity, it is warmed, moistened, and filtered by the nasal mucosa. The nasal cavity is surrounded by the paranasal sinuses in the frontal, sphenoid, ethmoid, and maxillary bones. These sinuses act as resonance chambers in speech and their mucosae, like that of the nasal cavity, warm and moisten the incoming air.
The nasal passages are separated from the oral cavity below by a partition composed anteriorly of the hard palate and posteriorly by the soft palate.
Pharynx
After passing through the nasal cavity, the air next reaches the pharynx (throat). There are three division of the pharynx: the nasopharynx, the oropharynx, and the laryngopharynx. The nasopharynx is the first division, and it is nearest to the nasal cavities. It contains the adenoids (also known as the pharyngeal tonsils), which are collections of lymphatic tissue. Below the nasopharynx and closer to the mouth is the second division of the pharynx, the oropharynx. In its lateral walls are the palatine tonsils, two rounded masses of lymphatic tissue. The lingual tonsil covers the base of the tongue. The third division of the pharynx is the laryngopharynx. It lies directly
posterior to the upright epiglottis and extends to the larynx, where the common pathway divides into the respiratory and digestive channels. From the laryngopharynx, air enters the lower respiratory passageways by passing through the larynx (voice box) and into the trachea below. Pharynx serves as a food and air passageway. Air enters from the nasal cavities and passes through the pharynx to the larynx. Food enters the pharynx from the mouth and passes into the esophagus.
Larynx
The larynx is the location of the vocal cords. It consists of nine cartilages. The two most prominent are the large shield-shaped thyroid cartilage, whose anterior medial laryngeal prominence is commonly referred to as Adam’s apple, and the inferiorly located, ring-shaped cricoid cartilage, whose wildest dimension faces posteriorly. A flap of cartilaginous tissue, the epiglottis, sits above the glottis. The epiglottis provides protection against food and liquid being inhaled into the lungs since it covers the larynx and trachea during swallowing.
Trachea
On its way to the lungs, air passes from the larynx to the trachea (windpipe), a vertical tube approximately 12.5 centimeters in length and 2.5 centimeters in diameter.
It extends downward in front of the esophagus and into the thoracic cavity, where it splits into right and left bronchi. Within the tracheal wall are about twenty C-shaped pieces of hyaline cartilage, one above the other. The open ends of these incomplete rings are directed posteriorly, and the gaps between their ends are filled with smooth muscle and connective tissues. The inner wall of the trachea is lined with a ciliated mucous membrane that contains many goblet cells. This membrane continues to filter the incoming air and to move entrapped particles upward into the pharynx where the mucus can be swallowed.
Bronchial Tubes
The distal end of the trachea divides to form the left and right main bronchi. Each bronchus enters one of the lungs and branches repeatedly to form secondary bronchi. Each branch becomes more narrow until the most narrow branches, the bronchioles, are formed. Each bronchiole terminates in a small group of air sacs, called alveoli. Each lung has approximately 150 million alveoli. A network of pulmonary capillaries from the pulmonary blood vessels tightly encases each alveolus. In fact, the walls of the alveoli and capillaries are so tightly associated with each other they are referred to as a single unit, the respiratory membrane. External respiration, the exchange of oxygen and carbon dioxide between the air within the alveolus and the blood inside the capillaries, takes place across the respiratory membrane.
Lungs
The lungs are soft, spongy, cone-shaped organs located in the thoracic cavity. The right and left lungs are separated medially by the mediastinum, and they are enclosed by the diaphragm and the thoracic cage.
Each lung is enveloped in a double-folded membrane called the pleura. The outer layer of the pleura, nearest the ribs, is the parietal pleura, and the inner layer, closest to the lung, is the visceral pleura. The pleura is moistened with a serous fluid that facilitates the movements of the lungs within the chest.
The right lung is slightly larger than the left one. It is divided into three lobes and the left lung is divided into two lobes. The uppermost part of the lung is called the apex, and the lower area is the base. The hilum of the lung is the midline region
where blood vessels, nerves, lymphatic tissue, and bronchial tubes enter and exit the organ. The area between the right and left lung is called the mediastinum. The mediastinum contains the heart, esophagus, thymus gland, and main bronchi.
Mechanics of Respiration
The lungs extend from the clavicle to the diaphragm in the thoracic cavity. The diaphragm is a muscular partition that separates the thoracic from the abdominal cavity and aids in the process of breathing. The diaphragm contracts and moves down into the abdominal cavity, which causes a decrease of pressure, or negative thoracic pressure, within the chest cavity. Air can then enter the lungs to equalize the pressure during inhalation. The intercostal muscles between the ribs assist inhalation by raising the rib cage to enlarge the thoracic cavity.
The diaphragm and intercostal muscles relax and the thoracic cavity becomes smaller, when pressure within the cavity increases and air is pushed out of the lungs, resulting in exhalation. Therefore, a quiet, unforced exhalation is a passive process since it does not require any muscle contraction.
Respiratory Volumes and Capacities
A person’s size, sex, age, and physical condition produce variations in respiratory volumes. Normal quiet breathing moves about 500 ml of air in and out of the lungs with each breath. On the average, the same amount leaves during a normal resting expiration. One inspiration plus the following expiration is called a respiratory cycle. Terminology relating to this measurement is listed below.
Tidal volume (TV): the amount of air that enters the lungs in a single inhalation or leaves the lungs in a single exhalation of quiet breathing. In an adult this is normally
500 cc.
Inspiratory reserve volume (IRV): the air that can be forcibly inhaled after a normal respiration has taken place. Also called complemental air, generally measures around 3,000 cc.
Expiratory reserve volume (ERV): the amount of air that can be forcibly exhaled after a normal quiet respiration. This is also called supplemental air, approximately 1,000 cc.
Residual volume: the air remaining in the lungs after a forced exhalation; about 1,500 cc in the adult.
Inspiratory capacity (IC): the volume of air inhaled after a normal exhale. Functional residual capacity (FRC): the air that remains in the lungs after a normal exhalation has taken place.
Vital capacity (VC):the total volume of air that can be exhaled after a maximum inhalation. This amount will be equal to the sum of TV, IRV, and ERV.
Total lung capacity (TLC): the volume of air in the lungs after a maximal inhalation. Respiratory Rate
The respiratory rate is one of our vital signs (VS), along with heart rate, temperature, and blood pressure. Respiratory rate is dependent on the level of CO2 in the blood. When the CO2 level is high, we breathe more rapidly to expel the excess. However, if CO2 levels drop, our respiratory rate will also drop.
When a respiratory rate falls outside the range of normal, it would indicate an illness or medical condition. For example, when a patient is running an elevated temperature and has shortness of breath (SOB) due to pneumonia, the respiratory rate may increase dramatically. However, some medications, pain medication in particular, can cause a decrease in the respiratory rate.
Respiratory Rates for Different Age Groups
Age Respirations per Minute
newborn 30-60
1-year-old 18-30
16-year-old 16-20
adult 12-20
Combining Forms Commonly Used in This System Combining form Meaning Example
adenoid/o adenoids adenoidectomy
alveol/o alveolus; air sac alveolar
bronch/o bronchus bronchoscope
bronchi/o bronchus bronchiectasis bronchiol/o bronchiole, small bronchiolitis
Bronchus
capn/o carbon dioxide acapnia
epiglott/o epiglottis epiglottitis
laryng/o larynx, voice box laryngospasm
lob/o lobe lobectomy
muc/o mucus mucus
nas/o nose nasopharynx
ox/o oxygen anoxia
pharyng/o pharynx pharyngeal tonsils
pleur/o pleura pleurocentesis
pneum/o air, lung pneumothorax
pneumon/o
pulmon/o lung pulmonology
rhin/o nose rhinorrhagia
sinus/o sinus, cavity pansinusitis
spir/o breathing spirometer
tonsill/o tonsils tonsillectomy
trache/o trachea, windpipe tracheotomy
thorac/o chest thoracalgia
Suffixes Commonly Used in This System
Suffixes Meaning Example
-capnia carbon dioxide hypercapnia
-ectasis stretching out, dilatation, bronchiectasis
expansion
-emia blood condition hypoxemia
-oxia oxygen anoxia
-pnea breathing dyspnea Diagnostic Procedures Relating to This System
chest X-ray taking a radiographic picture of the lungs and
heart from the back and sides.
chest CT(computed computerized images of the chest reproduced in
sections sliced
tomography) scan from front to back horizontally. Used to diagnose
tumors, abscesses, and pleural effusion. Computed
tomography is used to visualize other body parts
such as the abdomen and the brain.
pulmonary function tests(PFT) a group of diagnostic tests that give information
regarding air flow in and out of the lungs, lung
volumes, and gas exchange between the lungs and
bloodstream
tuberculin skin tests(TB test) applying a chemical agent (Tine or Mantourx tests)
under the surface of the skin to determine if the
patient has been exposed to tuberculosis. ventilation-perfusion scanning(VPS) a nuclear medicine procedure used to diagnose
pulmonary embolism and other condition.
Radioactive air is inhaled for the ventilation
portion to determine if air is filling the entire
lung. Radioactive intravenous injection shows
whether or not blood is flowing to all parts of
the lung.
Pathology
Bronchiectasis: Bronchiectasis is destruction and widening of the large airways.
A person may be born with it (congenital bronchiectasis) or may develop it later in life.
Bronchiectasis is often caused by recurrent inflammation or infection of the airways. It may be present at birth, but most often begins in childhood as a complication from infection or inhaling a foreign object.
Cystic fibrosis causes about 50% of all bronchiectasis in the United States today. Recurrent, severe lung infections (pneumonia, tuberculosis, fungal infections), abnormal lung defenses, and obstruction of the airway by a foreign body or tumor are some of the predisposing factors. It can also be caused by routinely breathing in food particles while eating.
Symptoms often develop gradually, and may occur months or years after the event that causes the bronchiectasis.
Symptoms include
●Chronic cough with large amounts of foul-smelling sputum production
●Coughing up blood
●Cough worsened by lying on one side
●Shortness of breath worsened by exercise
●Weight loss
●Fatigue
●Clubbing of fingers may be present (abnormal amount of tissue in the
fingernail beds)
●Wheezing
●Skin discoloration, bluish
●Paleness
●Breath odor
When listening to the chest with a stethoscope, the doctor may hear small clicking, bubbling, wheezing, rattling, or other sounds, usually in the lower lobes of the lungs. Tests may include:
●Chest x-ray
●Chest CT
●Sputum culture
●CBC
●Sweat test or other cystic fibrosis testing
●Serum Immunoglobulin analysis
●Serum precipitins (testing for antibodies to the fungus aspergillus)
●PPD (purified protein derivative) skin test for prior TB infection
Treatment is aimed at controlling infections and bronchial secretions, relieving airway obstruction, and preventing complications.
Antibiotics, bronchodilators, and expectorants are often prescribed for infections. Regular, daily drainage to remove bronchial secretions is a routine part of treatment.
A respiratory therapist can teach postural drainage and effective coughing exercises to patients and their families.
Surgical lung resection may be indicated for those who fail to respond to therapy or for massive bleeding.
Childhood vaccinations and a yearly influenza vaccine help reduce the chance of some infections. Avoiding upper respiratory infections, smoking, and pollution may lessen the susceptibility to infection.
Pneumonia: Pneumonia is an infection of the lungs. Many different organisms can cause it, including bacteria and viruses.
Pneumonia can range from mild to severe, and can even be deadly. The severity depends on the type of organism causing pneumonia, as well as your age and underlying health.
Bacterial pneumonia tends to be the most serious and, in adults, the most common cause of pneumonia. The most common pneumonia-causing bacterium in adults is Streptococcus pneumoniae(pneumococcus). In some people, particularly the elderly and those who are debilitated, bacterial pneumonia may follow influenza or even a common cold.
Respiratory viruses are the most common causes of pneumonia in young children, peaking between the ages of 2 and 3. By school age, the bacterium Mycoplasma pneumoniae becomes more common.
People who have trouble swallowing are at risk of aspiration pneumonia. In this condition, food, liquid, or saliva accidentally goes into the airways. It is more common in people who have had a stroke, Parkinson's disease, or previous throat surgery.
It is often harder to treat pneumonia in people who are in a hospital, or a nursing facility.
The main symptoms of pneumonia are:
●Cough with greenish or yellow mucus; bloody sputum happens on occasion
●Fever with shaking chills
●Sharp or stabbing chest pain worsened by deep breathing or coughing
●Rapid, shallow breathing
●Shortness of breath
Additional symptoms include:
●Headache
●Excessive sweating and clammy skin
●Loss of appetite
●Excessive fatigue
●Confusion, especially in older people
If you have pneumonia, you may be working hard to breathe, or may be breathing fast. Crackles are heard when listening to your chest with a stethoscope. Other abnormal breathing sounds may also be heard through the stethoscope or via percussion (tapping on your chest wall).The health care provider will likely order a chest x-ray if pneumonia is suspected.
Some patients may need other tests, including:
●Gram's stain and culture of your sputum to look for the organism causing your
symptoms
●CBC to check white blood cell count; if high, this suggests bacterial infection
●Arterial blood gases to check how well you are oxygenating your blood
●CAT scan of the chest
●Pleural fluid culture if there is fluid in the space surrounding the lungs
If the cause is bacterial, the doctor will try to cure the infection with antibiotics. If the cause is viral, typical antibiotics will NOT be effective. Sometimes, however, your doctor may use antiviral medication. It may be difficult to distinguish between viral and bacterial pneumonia, so you may receive antibiotics.
Many people can be treated at home with antibiotics. You can take these steps at home:
●Drink plenty of fluids to help loosen secretions and bring up phlegm.
●Get lots of rest. Have someone else do household chores.
●Control your fever with aspirin or acetaminophen. DO NOT give aspirin to
children.
If you have an underlying chronic disease, severe symptoms, or low oxygen levels, you will likely require hospitalization for intravenous antibiotics and oxygen therapy. Infants and the elderly are more commonly admitted for treatment of pneumonia. When in the hospital, respiratory treatments to remove secretions may be necessary. Occasionally, steroid medications may be used to reduce wheezing if there is an underlying lung disease.
Emphysema: Emphysema is a condition in which the walls between the alveoli or air sacs within the lung lose their ability to stretch and recoil. The air sacs become weakened and break. Elasticity of the lung tissue is lost, causing air to be trapped in the air sacs and impairing the exchange of oxygen and carbon dioxide. Also, the support of the airways is lost, allowing for airflow obstruction.
Symptoms of emphysema include shortness of breath, cough and a limited exercise tolerance. Emphysema and chronic bronchitis frequently co-exist together to comprise chronic obstructive pulmonary disease (COPD). COPD does not include other obstructive lung diseases such as asthma.
Cigarette smoking is by far the most common cause of emphysema. Smoking is responsible for approximately 80-90% of deaths due to COPD.1
In addition, in the absence of alpha 1-antitrypsin (AAT), an inherited form of emphysema called alpha 1-antitrypsin deficiency related emphysema is almost inevitable. Symptoms of AAT deficiency emphysema usually begin between 32 and
41 years of age. Smoking significantly increases the severity of emphysema in AAT-deficient individuals.
Emphysema doesn't develop suddenly. It comes on very gradually. Years of exposure to the irritation of cigarette smoke usually precede the development of emphysema.
The goal of treatment is to provide relief of symptoms and prevent progression of the disease with a minimum of side effects. The doctor's advice and treatment may include:
●Quitting smoking: the single most important factor for maintaining healthy
lungs.
●Bronchodilator drugs (prescription drugs that relax and open air
passages in the lungs): may be prescribed to treat emphysema if there is a tendency toward airway constriction or tightening. These drugs may be inhaled as aerosol sprays or taken orally.
●Antibiotics: if you have a bacterial infection, such as pneumococcal
pneumonia.
●Steroids: these may be used for relapses or "acute exacerbations."
●Exercise: including breathing exercises to strengthen the muscles used in
breathing as part of a pulmonary rehabilitation program to condition the rest of the body.
●Alpha 1-Proteinase Inhibitor (A1PI): only if a person has AAT
deficiency-related emphysema. A1PI is not recommended for those who develop emphysema as a result of cigarette smoking or other environmental factors.
●Lung transplantation: a major procedure, which can be effective.
●Lung volume reduction surgery: a surgical procedure in which the most
severely diseases portions of the lung are removed to allow the remaining lung and breathing muscles to work better. The short-term results are promising but those with severe forms are at higher risk of death.
Continuing research is being done to find answers to prevent the disease.
Quitting smoking can prevent the occurrence and decrease the progression of emphysema. Maintain overall good health habits, which include proper nutrition, adequate sleep, and regular exercise to build up your stamina and resistance to infections.
Reduce your exposure to air pollution, which may aggravate symptoms of emphysema. On days when the ozone (smog) level is unhealthy, restrict your activity to early morning or evening. When pollution levels are dangerous, remain indoors and stay as comfortable as possible.
Consult your doctor at the start of any cold or respiratory infection because infection can make your emphysema symptoms worse. Ask about getting vaccinated against influenza and pneumococcal pneumonia.
Vocabularies
acute exacerbations[????◆??] [?????????????????]急性转剧,
急性加重
adenoidectomy[ ??????????????]腺样体切除术
adenoids[ ????????]腺样增殖体
aerosol sprays[ ??????●][?????]喷雾剂
airway Constriction[ ???????????]气道狭窄
alpha 1-antitrypsin (AAT) α1抗胰蛋白酶
alpha 1-Proteinase Inhibitor (A1PI)
[ ???◆??????][??????????
??] α1解蛋白酶抑制剂
alveoli[?●????●??]气泡
apex[ ??????] (复apexes apices)尖,顶端,螺顶,翅尖,叶尖
aspiration pneumonia[ ???????????][??◆??????◆???]吸入
性肺炎
auditory tube[ ????????][ ??◆??]耳咽管,咽鼓管
base[????]基底
bronchial tubes[ ???????●][ ??◆??]小支气管
bronchioles[ ???????◆●]细支气管
bronchodilator drugs[ ???????????●????]支气管扩张药bronchodilator[ ???????????●????]支气管扩张剂
bronchus[ ???????]支气管
carbon dioxide [ ??????][??????????]二氧化碳
chronic obstructive pulmonary disease (COPD) [ ??●??????]慢性阻塞性肺
病
cilia[ ??●??]纤毛; 细毛
clammy skin[ ?●???][????]冷湿皮肤
clubbing [ ?●????]杵状变
collarbone [???●?????]锁骨
congenital [ ?????????●]先天性的
crackles[ ????●?]湿罗音
cricoid cartilage [ ????????][ ?????●???]环状软骨
cystic fibrosis [ ??????][???????◆???]纤维囊泡症
diaphragm [ ????????]隔膜
epiglottis[ ?????●????]会厌
esophagus [????????????]食管,食道
ethmoid bone[ ??????][??◆?]筛骨
eustachian tube[ ◆??????????][ ??◆??]欧氏管,咽鼓管exhalation[ ??????●?????]呼出
expectorants[?????????????]祛痰剂
expiration[ ??????????????]呼出
frontal bone [ ?????●][??◆?]额骨
fungal infections[ ?????●][?????????] 霉菌感染
fungi[ ???????]真菌,霉菌
glottis[ ?●????]声门
goblet cell [ ???●??] [??●]杯状细胞,杯形细胞
Gram's stain[????][?????]革兰(氏)染色
hilum[ ???●??]门
hyaline cartilage [ ????●???][ ?????●???]透明软骨immunoglobulin[????◆???◆??●???◆●??]免疫球蛋白
inhalation[ ?????●?????]吸入
inspiration [ ????????????] 吸(气),吸气
laryngopharynx[●????????????????]喉咽
larynx[ ●??????]喉
lingual tonsil[ ●?????●][ ?????●]舌扁桃体
lung resection[●??][?????????]肺切除(术)
lung volume reduction surgery[ ????????]肺减容积手术
lung[●??]肺
maxillary bone[??????●???][??◆?]上颌骨
mediastinum[ ??????????????]纵隔
metabolism[???????●????]新陈代谢,代谢作用
mucous membrane[ ??◆????][ ????????]粘膜
mucus[ ??◆??? ?]粘液
mycoplasma pneumoniae
[ ?????◆??●????][??◆???
??◆???]肺炎支原体
nares[ ???????]鼻孔
nasal cavity[ ?????●?][ ?????]鼻腔
nasal conchae [ ?????●][ ?????]鼻甲
nasal septum[ ?????●][ ??????]鼻中隔
nasopharynx[ ?????◆????????]鼻咽
nose[??◆?]鼻
organisms[ ?????????]有机体
oropharynx[ ?◆??????????]口咽
oxygen[ ????????]氧(双原子气态氧),氧,氧气
palate[ ??●??]腭
palatine tonsil[ ??●?????][ ?????●]腭扁桃体
paranasal sinus[ ??????????●][ ??????]鼻旁窦
parietal pleura[?????????●][ ?●◆???]胸膜壁层
Parkinson's disease[ ????????????]震颤(性假)麻痹,帕金森(氏)病percussion[?????????]叩诊
pharyngeal tonsil[ ???????????●] [ ?????●]咽扁桃体
pharynx[ ???????]咽
phlegm[?●??]粘液,粘痰
pleura[ ?●◆???]胸膜
pleural cavity[ ?●◆???●][ ??????]胸膜腔
pneumococcal pneumonia[ ??◆??????????●]
[??◆??????◆???]肺炎球菌性肺炎predisposing factor[ ??????????◆?][ ?????]易感因素,患病因素pulmonary capillaries[ ??●??????][ ????●???]肺毛细血管
relapses[???●???]复发,再发
respiratory membrane[??????????????][ ????????]呼吸膜serous fluid[ ??????][ ?●◆?????]浆液
shield-shaped [???●? ?????]盾形的
sphenoid bone[ ????????] [??◆?]蝶骨
stabbing[ ??????]刺穿的
stethoscope[ ????????◆?]听诊器
streptococcus pneumoniae[ ???????◆??????]
[??◆??????◆???] (pneumococcus)
肺炎球菌
thyroid cartilage[ ???????][ ?????●???]甲状软骨
tonsillectomy[ ??????●??????]扁桃体切除术
trachea[????????]气管
tuberculin skin tests [??◆?????????◆●??][????][ ????]结核
菌素皮肤试验:检结核病
ventilation-perfusion scanning
[ ?????●?????????????◆?
???][ ??????]通气灌注扫描
visceral pleura[ ??????●][ ?●◆???]脏胸膜
vocal cords[ ??◆?●][ ????]声带
wheeze [???????]喘鸣,哮鸣
Exercises and Answers
I.Match the terms in the first column with the correct definitions in the second
column.
_____1. alveoli a. tubes carrying air between the trachea and lungs
_____2. bronchi b. passageway for air to the bronchi
_____3. larynx c. located in the thoracic cavity
_____4. lungs d. membrane covering the lung
_____5. pharynx e. lymphoid tissue behind the nasal cavity
_____6. pleura f. acts as food and air passage
_____7. adenoids g. location of the vocal cords
_____8. trachea h. air sacs at the end of the bronchioles
i. keeps food out of the trachea and larynx
II.Define the following combining forms.
1.bronch/o______________________________________________________
2.rhin/o_____________________________________________________
3.pneumon/o__________________________________________________
https://www.wendangku.net/doc/7a10882958.html,ryng/o____________________________________________________
5.epiglott/o____________________________________________________
6.tonsil/o_____________________________________________________
7.lob/o________________________________________________________
8.pleur/o_______________________________________________________
9.pulmon/o______________________________________________________
10.alveol/o_______________________________________________________
11.adenoid/o______________________________________________________
12.sinus/o________________________________________________________
13.thorac/o_______________________________________________________
14.spir/o_________________________________________________________
15.muc/o_________________________________________________________ III.State the terms described using the combining forms provided.
1. discharge from the nose__________________________________________
2.inflammation of the larynx________________________________________
3.visual examination of the larynx____________________________________
4.bronchial rapid flow______________________________________________
5.spasm of the bronchus_____________________________________________
6.surgical repair of the chest__________________________________________
7.chest pain_______________________________________________________
8.cutting into the trachea_____________________________________________
9.narrowing of the trachea____________________________________________
10.suture the trachea__________________________________________________ IV.Match the suffixes in the first column with their correct definitions in the second column.
______1. -oxia a. chest
_______2. -thorax b. carbon dioxide
_______3. -stenosis c. blood condition
_______4. -pnea d. stretching out, dilatation, expansion
_______5. -emia e. surgical puncture to aspirate fluid
_______6. -algia f. oxygen
_______7. -ectasis g. breathing
_______8. -centesis h. constriction or narrowing
_______9. -capnia i. pain
V. Define each suffix and use it to form a term from the respiratory system.
Meaning Respiratory Term
1. -algia _________ ______________
2. –capnia _________ _______________
3. –centesis _________ _______________
4. –emia __________ _______________
5. –pnea __________ _______________
6. –stenosis ___________ ________________
7. –ectasis __________ ________________
VI. Match the diseases with the descriptions
bronchiectasis pneumonia emphysema
1. It is a condition in which the walls between the alveoli or air sacs within the lung lose their ability to stretch and recoil. The air sacs become weakened and
break. Elasticity of the lung tissue is lost, causing air to be trapped in the air sacs and impairing the exchange of oxygen and carbon dioxide.__________
2. It is the destruction and widening of the large airways. It is often caused by recurrent inflammation or infection of the airways. It may be present at birth, but most often begins in childhood as a complication from infection or inhaling a foreign object._____________
3. It is an infection of the lungs. Many different organisms can cause it, including bacteria, viruses, and fungi.It can range from mild to severe, and can even be deadly. The severity depends on the type of organism causing it, as well as the age and underlying health. The most common causing bacterium in adults is pneumococcus.___________
Answer:
I.h a g c f d e b
II. 1.bronchus 2.nose 3.lung or air https://www.wendangku.net/doc/7a10882958.html,rynx 5.epiglottis 6.tonsil
7.lobe 8.pleura 9.lung 10.alveolus or air sac 11.adenoids 12.sinus,
cavity 13.chest 14.breathing 15.mucus
III.rhinorrhea https://www.wendangku.net/doc/7a10882958.html,ryngitis https://www.wendangku.net/doc/7a10882958.html,ryngoscopy 4.bronchorrhagia
5.bronchospasm
6.thoracoplasty
7.thoracalgia
8.tracheotomy
9.tracheostenosis 10.tracheorrhaphy
IV. f a h g c i d e b
1.pain; thoracalgia
2.carbon dioxide; hypercapnia
3.surgical puncture to aspirate fluid; pleurocentesis
4.blood condition; hypoxemia
5.breathing; dyspnea
V. 6. constriction or narrowing; tracheostenosis 7. stretching out, dilatation, expansion; bronchiectasis
VI.emphysema bronchiectasis pneumonia
Reading Practice
Pulmonology Consultation Report
Reason for Consultation: Evaluation o f inc reasingly severe asthma.
History of Present Illness: Patient is currently a 10-year-old male who first presented to the Emergency Room with dyspnea, coughing, and wheezing at 7 years of age. Paroxysmal attacks are increasing in frequency and there do not appear to be any precipitating factors such as exercise. No other family members are asthmatics. Results of Physical Examination: Patient is currently in the ER with a paroxysmal attack with marked dyspnea, cyanosis around the lips, prolonged expiration, and a hacking cough producing thick, nonpurulent phlegm. Thoracic auscultation with stethoscope revealed rhonchi throughout bilateral lung fields. Chest X-ray shows poor pulmonary expansion, with hypoxemia indicated by ABG. A STAT pulmonary function test reveals moderately severe airway obstruction during expiration. This
patient responded to oxygen therapy and IV Alupent and steroids, and he is beginning to cough less and breathe with less effort.
Assessment: Acute asthma attack with evere airway obstruction. There is no evidence of pulmonary infection. In view of increasing severity and frequency of attacks, all his medicatiions should be reevaluated for effectiveness and all attempts to identify precipitating factors should be made.
Recommendations: Patient is to continue to use Alupent for relief of bronchospasms and steroids to reduce general inflammation. Instructions for taking medications and controlling severity of asthma attacks were carefully reviewed with the patient and his family. A referral to an allergist was made to evaluate this young man for presence of environmental allergies.
Critical Thinking Questions
1.What does the medical term paroxysmal mean?
2.What do the following abbreviations stand for?
a.IV
b.STAT
c.ABG
3.The patient was discharged and sent home with two medications. Explain in your
own words the purpose of each of these medications.
4.What important informatiion regarding this young man’s asthma is unknown to
the physician? What does this consulting physician recommend to address this problem?
5.Describe the characteristics related to t his patient’s cough in your own words.
6.Which of the following is not one of the symptoms seen in the emergency room?
a.crackling lung sounds
b.bluish skin
c.difficulty breathing
d.extended breathing out time
Vocabulary
Alupent [ ?●?◆?????]硫酸异丙喘宁
auscultation[ ?????●???????] 听诊
cyanosis [ ???????◆???]发绀,青紫
dyspnea [?????????]呼吸困难
hacking cough[ ?????] 干咳
hypoxemia [ ?????????????]低氧血,低氧血症
purulent [ ??????●???]化脓的,脓性的,化脓性的
paroxysmal attacks[ ???????????●][?????] 发作的,阵发的precipitating factors[??????????????] 促发因素
rhonchus[ ??????] (pl. rhonchi)干啰音
03第三讲 吸声处理
噪声治理课程第三讲吸声处理 一、吸声 1.1 吸声系数与降噪系数 吸声是声波撞击到材料表面后能量损失的现象,吸声可以降低室内声压级。描述吸声的指标是吸声系数α,代表被材料吸收的声能与入射声能的比值。理论上,如果某种材料完全反射声音,那么它的α=0;如果某种材料将入射声能全部吸收,那么它的α=1。事实上,所有材料的α介于0和1之间,也就是不可能全部反射,也不可能全部吸收。 不同频率上会有不同的吸声系数。人们使用吸声系数频率特性曲线描述材料在不同频率上的吸声性能。按照ISO标准和国家标准,吸声测试报告中吸声系数的频率范围是100-5KHz。将100-5KHz的吸声系数取平均得到的数值是平均吸声系数,平均吸声系数反映了材料总体的吸声性能。在工程中常使用降噪系数NRC粗略地评价在语言频率范围内的吸声性能,这一数值是材料在250、500、1K、2K四个频率的吸声系数的算术平均值,四舍五入取整到0.05。一般认为NRC小于0.2的材料是反射材料,NRC大于等0.2的材料才被认为是吸声材料。当需要吸收大量声能降低室内混响及噪声时,常常需要使用高吸声系数的材料。如离心玻璃棉、岩棉等属于高NRC吸声材料,5cm厚的24kg/m3的离心玻璃棉的NRC可达到0.95。 测量材料吸声系数的方法有两种,一种是混响室法,一种是驻波管法。混响室法测量声音无规入射时的吸声系数,即声音由四面八方射入材料时能量损失的比例,而驻波管法测量声音正入射时的吸声系数,声音入射角度仅为90度。两种方法测量的吸声系数是不同的,工程上最常使用的是混响室法测量的吸声系数,因为建筑实际应用中声音入射都是无规的。在某些测量报告中会出现吸声系数大于1的情况,这是由于测量的实验室条件等造成的,理论上任何材料吸收的声能不可能大于入射声能,吸声系数永远小于1。任何大于1的测量吸声系数值在实际声学工程计算中都不能按大于1使用,最多按1进行计算。 在房间中,声音会很快充满各个角落,因此,将吸声材料放置在房间任何表面都有吸声效果。吸声材料吸声系数越大,吸声面积越多,吸声效果越明显。可以利用吸声天花、吸声墙板、空间吸声体等进行吸声降噪。 1.2吸声原理 纤维多孔吸声材料,如离心玻璃棉、岩棉、矿棉、植物纤维喷涂等,吸声机理是材料内部有大量微小的连通的孔隙,声波沿着这些孔隙可以深入材料内部,与材料发生摩擦作用将声能转化为热能。多孔吸声材料的吸声特性是随着频率的增高吸声系数逐渐增大,这意味着低频吸收没有高频吸收好。多孔材料吸声的必要条件是:材料有大量空隙,空隙之间互相连通,孔隙深入材料内部。错误认识之一是认为表面粗糙的材料具有吸声性能,其实不然,例如拉毛水泥、表面凸凹的石才基本不具有吸声能力。错误认识之二是认为材料内部具有大量孔洞的材料,如聚苯、聚乙烯、闭孔聚氨脂等,具有良好的吸声性能,事实上,这些材料由于内部孔洞没有连通性,声波不能深入材料内部振动摩擦,因此吸声系数很小。 与墙面或天花存在空气层的穿孔板,即使材料本身吸声性能很差,这种结构也具有吸声性能,如穿孔的石膏板、木板、金属板、甚至是狭缝吸声砖等。这类吸声被称为亥姆霍兹共振吸声,吸声原理类似于暖水瓶的声共振,材料外部空间与内部腔体通过窄的瓶颈连接,声波入射时,在共振频率上,颈部的空气和内部空间之间产生剧烈的共振作用损耗了声能。亥姆霍兹共振吸收的特点是只有在共振频率上具有较大的吸声系数。 薄膜或薄板与墙体或顶棚存在空腔时也能吸声,如木板、金属板做成的天花板或墙板等,这种结构的吸声机理是薄板共振吸声。在共振频率上,由于薄板剧烈振动而大量吸收声能。薄板共振吸收大多在低频具有较好的吸声性能。 二、吸声材料及吸声结构
图像处理课后习题
第一章绪论 1. 模拟图像处理与数字图像处理主要区别表现在哪些方面? (什么是图像?什么是数字图像?什么是灰度图像?模拟图像处理与数字图像处理主要区别表现在哪些方面?) 图像:是对客观对象的一种相似性的、生动性的描述或写真。 数字图像:一种空间坐标和灰度均不连续的、用离散数字(一般用整数)表示的图像。 灰度图像:在计算机领域中,灰度数字图像是每个像素只有一个采样颜色的图像。在数字图像领域之外,“黑白图像”也表示“灰度图像”,例如灰度的照片通常叫做 “黑白照片”。 模拟图像处理与数字图像处理主要区别:模拟图像处理是利用光学、照相方法对模拟图像的处理。(优点:速度快,一般为实时处理,理论上讲可达到光的速度, 并可同时并行处理。缺点:精度较差,灵活性差,很难有判断能力和非线性处理能力) 数字图像处理(称计算机图像处理,指将图像信号转换成数字格式并利用计算机对数据进行处理的过程)是利用计算机对数字图像进行系列操作,从而达到某种预期目的的技术.(优点:精度高,内容丰富,可进行复杂的非线性处理,灵活的变通能力,一只要改变软件就可以改变处理内容) 2. 图像处理学包括哪几个层次?各层次间有何区别和联系? 数字图像处理可分为三个层次:狭义图像处理、图像分析和图像理解。狭义图像处理是对输入图像进行某种变换得到输出图像,是一种图像到图像的过程。 图像分析主要是对图像中感兴趣的目标进行检测和测量,从而建立对图像目标的描述,图像分析是一个从图像到数值或符号的过程。 图像理解则是在图像分析的基础上,基于人工智能和认知理论研究图像中各目标的性质和它们之间的相互联系,对图像内容的含义加以理解以及对原来客观场景加以解译,从而指导和规划行动。 区别和联系:狭义图像处理是低层操作,它主要在图像像素级上进行处理,处理的数据量非常大;图像分析则进入了中层,经分割和特征提取,把原来以像素构成的图像转变成比较简洁的、非图像形式的描述;图像理解是高层操作,它是对描述中抽象出来的符号进行推理,其处理过程和方法与人类的思维推理有许多类似之处。 3. 图像处理与计算机图形学的区别与联系是什么? 数字图像处理,是指有计算机及其它有关的数字技术,对图像施加某种运算和处理,从而达到某种预期的目的,而计算机图形学是研究采用计算机生成,处理和显示图形的一门科学。 二者区别:研究对象不同,计算机图形学研究的研究对象是能在人的视觉系统中产生视觉印象的事物,包括自然景物,拍摄的图片,用数学方法描述的图形等,而数字图像处理研究对象是图像;研究内容不同,计算机图像学研究内容为图像生成,透视,消阴等,而数字图像处理研究内容为图像处理,图像分割,图像透析等;过程不同,计算机图像学是由数学公式生成仿真图形或图像,而数字图像处理是由原始图像处理出分析结果,计算机图形与图像处理是逆过程。 结合每个人的本专业学科、工作应用,谈谈数字图像处理的关系或在本专业学科中的应用。 检测技术与自动化装置是把自动化、电子、计算机、控制工程、信息处理、机械等多种
进行识别前图像预处理
进行识别前图像预处理 //BP神经网络字符识别函数定义 #include "dibapi.h" #include <iostream> #include <deque> #include <math.h> using namespace std; typedef deque<CRect> CRectLink; typedef deque<HDIB> HDIBLink; //声明一些必要的全局变量 int w_sample=8; int h_sample=16; bool fileloaded; bool gyhinfoinput; bool gyhfinished; int digicount; int m_lianXuShu; CRectLink m_charRectCopy; CRectLink m_charRect; HDIBLink m_dibRect; HDIBLink m_dibRectCopy;
HDIB m_hDIB; CString strPathName; CString strPathNameSave; /********************************function declaration*************************************/ //清楚屏幕 void ClearAll(CDC* pDC); //在屏幕上显示位图 void DisplayDIB(CDC* pDC,HDIB hDIB); //对分割后的位图进行尺寸标准归一化 void StdDIBbyRect(HDIB hDIB, int tarWidth, int tarHeight); //整体斜率调整 void SlopeAdjust(HDIB hDIB); //去除离散噪声点 void RemoveScatterNoise(HDIB hDIB); //梯度锐化 void GradientSharp(HDIB hDIB); //画框 void DrawFrame(CDC* pDC,HDIB hDIB, CRectLink charRect,unsigned int linewidth,COLORREF color); //将灰度图二值化 void ConvertGrayToWhiteBlack(HDIB hDIB);
数字图像处理第三版第五章答案
第五章 一个带通滤波通过从相应的带阻滤波而获得: 然后: (a)理想带通滤波: (b)巴特带通滤波: (c)高斯带通滤波:
带阻滤波器公式可以通过带通滤波器的公式得到。两者的和为1. ),(1),(v u H v u H np nr -= 然后: (a) 理想带阻滤波: { 01),(= v u H 2.巴特带阻滤波: 我不想输这个公式了,这个就是下面的巴特带通滤波的公式中1减的后面那个式子 (b) 巴特带通滤波: 3.高斯带阻滤波: 我不想输这个公式了,这个就是下面的高斯带通滤波的公式中1减的后面中括号那个式子 (c)高斯带通滤波:
二维连续余弦函数的傅里叶变换 dxdy e y v x u A dxdy e v u f v u F vy ux j vy ux j )(200)(2)cos(),(),(+-+-????+==ππ 余弦的变换 )(2 1cos θθ θj i e e -+= 带入得到 ] [2][2][2 ),()(2)2/2/(2)(2)2/2/(2) (2)()(00000000??????+-+-+-++-+-+--=+- =dxdy e e A dxdy e e A dxdy e e e A v u F vy ux j y v x u j vy ux j y v x u j vy ux j y v x u j y v x u j πππππππππ 这些都是傅里叶变换的功能 并且 结果变换成 )]2,2()2,2([2),(0000π πδππδv v u u v v u u A v u F ++---- =即可
图像预处理的一般方法
图像预处理的一般方法 (一)空域图像增强技术 1.灰度线性变换 addpath('C:\'); I = imread('C:\lzs.jpeg'); imshow(I); I = double(I); [M,N] = size(I); for i = 1:M for j = 1:N if I(i,j)<=30 I(i,j)=I(i,j); else if I(i,j)<=150 I(i,j)=(210-30)/(160-30)*(I(i,j)-30)+30; else I(i,j)=(256-210)/(256-160)*(I(i,j)-160)+210; end end end end figure(2); imshow(uint8(I)); 2.直方图均衡化 addpath('C:\'); I=imread('C:\lzs.jpeg'); figure subplot(221); imshow(I);
subplot(222); imhist(I); I1=histeq(I); figure; subplot(221); imshow(I1); subplot(222); imhist(I1) 3.均值滤波 function test1 I = imread('C:\lzs.jpeg'); [M,N]=size(I); II1=zeros(M,N); for i=1:16; II(:,:,i)=imnoise(I,'gaussian',0,0.01); II1=II1+double(II(:,:,i)); if or(or(i==1,i==4),or(i==8,i==16)); figure;imshow(uint8(II1/i)); end end 4.梯度锐化操作 addpath('C:\'); I = imread('C:\lzs.jpeg'); subplot(131); imshow(I); H=fspecial('Sobel'); H=H'; TH=filter2(H,I); subplot(132); imshow(TH,[]);
图像预处理的主要方案
图像预处理的主要方案 1引言模拟世界的影像要为计算机系统所处理和理解一般要经过图像采集、图像预处理、特征取样、匹配分析等阶段。由于获取图像的工具或手段的影响成像系统获取的图像即原始图像由于受到种种条件限制和随机干扰往往不能直接使用必须在视觉信息处理的早期阶段对原始图像进行灰度校正、噪声过滤等图像预处理使获取图像无法完全体现原始图像的全部信息。因此对图像进行预处理就显得非常重要。预处理的目的是改善图像数据抑制不需要的变形或者增强某些对于后续处理来说比较重要的图像特征。 图1图像处理的输入输出简图在图像分析中对输入图像进行特征抽取、分割和匹配前所进行的处理。图像预处理的主要目的是消除图像中无关的信息恢复有用的真实信息增强有关信息的可检测性和最大限度地简化数据从而改进特征抽取、图像分割、匹配和识别的可靠性。预处理过程一般有数字化、几何变换、归一化、平滑、复原和增强等步骤。 2数字化一幅原始照片的灰度值是空间变量位置的连续值的连续函数。在M ×N点阵上对照片灰度采样并加以量化归为2b个灰度等级之一可以得到计算机能够处理的数字图像。为了使数字图像能重建原来的图像对M、N和b值的大小就有一定的要求。在接收装置的空间和灰度分辨能力范围内M、N和b的数值越大重建图像的质量就越好。当取样周期等于或小于原始图像中最小细节周期的一半时重建图像的频谱等于原始图像的频谱因此重建图像与原始图像可以完全相同。由于M、N和b三者的乘积决定一幅图像在计算机中的存储量因此在存储量一定的条件下需要根据图像的不同性质选择合适的M、N和b值以获取最好的处理效果。 3几何变换用于改正图像采集系统的系统误差和仪器位置的随机误差所进行的变换。对于卫星图像的系统误差如地球自转、扫描镜速度和地图投影等因素所造成的畸变可以用模型表示并通过几何变换来消除。随机误差如飞行器姿态和高度变化引起的误差难以用模型表示出来所以一般是在系统误差被纠正后通过把被观测的图和已知正确几何位置的图相比较用图中一定数量的地面控制点解双变量多项式函数组而达到变换的目的。 4归一化使图像的某些特征在给定变换下具有不变性质的一种图像标准形式。图像的某些性质例如物体的面积和周长本来对于坐标旋转来说就具有不变的性质。在一般情况下某些因素或变换对图像一些性质的影响可通过归一化处理得到消除或减弱从而可以被选作测量图像的依据。例如对于光照不可控的遥感图片灰度直方图的归一化对于图像分析是十分必要的。灰度归一化、几何归一化和变换归一化是获取图像不变性质的三种归一化方法。 5平滑消除图像中随机噪声的技术。对平滑技术的基本要求是在消去噪声的同时不使图像轮廓或线条变得模糊不清。常用的平滑方法有中值法、局部求平均法和k近邻平均法。局部区域大小可以是固定的也可以是逐点随灰度值大小变化的。此外有时应用空间频率域带通滤波方法。 6复原校正各种原因所造成的图像退化使重建或估计得到的图像尽可能逼近于理想无退化的像场。在实际应用中常常发生图像退化现象。例如大气流的扰动光学系统的像差相机和物体的相对运动都会使遥感图像发生退化。基本的复原技术是把获取的退化图像gxy看成是退化函数hxy和理想图像fxy的卷积。它们的傅里叶变换存在关系GuvHuvFuv。根据退化机理确定退化函数后就可从此关系式求出Fuv再用傅里叶反变换求出fxy。通常把称为反向滤波器。实际应用时由
图像预处理流程
图像预处理流程: 系统功能的实现方法 系统功能的实现主要依靠图像处理技术,按照上面的流程一一实现,每一部分的具体步骤如下: 1原始图像:由数码相机或其它扫描装置拍摄到的图像; 2预处理:对采集到的图像进行灰度化、图像增强,滤波、二值化等处理以克服图像干扰; 3字轮定位:用图像剪切的方法获取仪表字轮; 4字符分割:利用字符轮廓凹凸检测定位分割方法得到单个的字符; 5字符识别:利用模板匹配的方法与数据库中的字符进行匹配从而确认出字符,得到最后的仪表示数。 2.3.1 MATLA B简介 MATLAB是美国MathWorks公司出品的商业数学软件,用于算法开发、数据可视化、数据分析以及数值计算的高级技术计算语言和交互式环境,主要包括MATLAB 和Simulink两大部分。 MATLAB是矩阵实验室(Matrix Laboratory)的简称,和Mathematica、Maple 并称为三大数学软件。它在数学类科技应用软件中在数值计算方面首屈一指。MATLAB可以进行矩阵运算、绘制函数和数据、实现算法、创建用户界面、连接其他编程语言的程序等,主要应用于工程计算、控制设计、信号处理与通讯、图像处理、信号检测、金融建模设计与分析等领域。 MATLAB的基本数据单位是矩阵,它的指令表达式与数学、工程中常用的形式十分相似,故用MATLAB来解算问题要比用C,FORTRAN等语言完相同的事情简捷得多,并且mathwork也吸收了像Maple等软件的优点,使MATLAB成为一个强大的数学软件。在新的版本中也加入了对C,FORTRAN,C++ ,JAVA的支持。可以
直接调用,用户也可以将自己编写的实用程序导入到MATLAB函数库中方便自己以后调用,此外许多的MATLAB爱好者都编写了一些经典的程序,用户可以直接进行下载就可以用。 2.3.2 MATLAB的优势和特点 1、MATLAB的优势 (1)友好的工作平台和编程环境 MATLAB由一系列工具组成。这些工具方便用户使用MATLAB的函数和文件,其中许多工具采用的是图形用户界面。包括MATLAB桌面和命令窗口、历史命令窗口、编辑器和调试器、路径搜索和用于用户浏览帮助、工作空间、文件的浏览器。随着MATLAB的商业化以及软件本身的不断升级,MATLAB的用户界面也越来越精致,更加接近Windows的标准界面,人机交互性更强,操作更简单。而且新版本的MATLAB提供了完整的联机查询、帮助系统,极大的方便了用户的使用。简单的编程环境提供了比较完备的调试系统,程序不必经过编译就可以直接运行,而且能够及时地报告出现的错误及进行出错原因分析。 (2)简单易用的程序语言 MATLAB是一种高级的矩阵/阵列语言,它包含控制语句、函数、数据结构、输入和输出和面向对象编程特点。用户可以在命令窗口中将输入语句与执行命令同步,也可以先编写好一个较大的复杂的应用程序(M文件)后再一起运行。新版本的MATLAB语言是基于最为流行的C++语言基础上的,因此语法特征与C++语言极为相似,而且更加简单,更加符合科技人员对数学表达式的书写格式。使之更利于非计算机专业的科技人员使用。而且这种语言可移植性好、可拓展性极强,这也是MATLAB能够深入到科学研究及工程计算各个领域的重要原因。 (3)强大的科学计算机数据处理能力 MATLAB是一个包含大量计算算法的集合。其拥有600多个工程中要用到的数学运算函数,可以方便的实现用户所需的各种计算功能。函数中所使用的算法都是科研和工程计算中的最新研究成果,而前经过了各种优化和容错处理。在通常情况下,可以用它来代替底层编程语言,如C和C++ 。在计算要求相同的情况下,使用MATLAB的编程工作量会大大减少。MATLAB的这些函数集包括从最简单最基本的函数到诸如矩阵,特征向量、快速傅立叶变换的复杂函数。函数所能解决的问题其大致包括矩阵运算和线性方程组的求解、微分方程及偏微分方程的组的求解、符号运算、
图像预处理技术
图像预处理 一般情况下,成像系统获取的图像(即原始图像)由于受到种种条件限制和随机干扰,往往不能在视觉系统中直接使用,必须在视觉信息处理的早期阶段对原始图像进行灰度校正、噪声过滤等图像预处理.对机器视觉系统来说,所用的图像预处理方法并不考虑图像降质原因,只将图像中感兴趣的特征有选择地突出,衰减其不需要的特征,故预处理后的输出图像并不需要去逼近原图像.这类图像预处理方法统称为图像增强.图像增强技术主要有两种方法:空间域法和频率域法.空间域方法主要是在空间域内对图像像素直接运算处理.频率域方法就是在图像的某种变换域,对图像的变换值进行运算,如先对图像进行付立叶变换,再对图像的频谱进行某种计算(如滤波等),最后将计算后的图像逆变换到空间域.本章首先讨论直方图修正方法,然后介绍各种滤波技术,其中,高斯平滑滤波器将作比较深入的讨论. 5.1直方图修正 许多图像的灰度值是非均匀分布的,其中灰度值集中在一个小区间内的图像是很常见的(图5.2(a )所示的对比度很弱的图像).直方图均衡化是一种通过重新均匀地分布各灰度值来增强图像对比度的方法.经过直方图均衡化的图像对二值化阈值选取十分有利.一般来说,直方图修正能提高图像的主观质量,因此在处理艺术图像时非常有用. 直方图修正的一个简单例子是图像尺度变换:把在灰度区间],[b a 内的像素点映射到 [,]z z k 1区间. 一般情况下,由于曝光不充分,原始图像灰度区间],[b a 常常为空间[,]z z k 1的子空间,此时,将原区间内的像素点z 映射成新区间内像素点'z 的函数表示为 z z z b a z a z k '()= ---+1 1 (5.1) 上述函数的曲线形状见图5.1(a).上述映射关系实际上将],[b a 区间扩展到区间[,]z z k 1上,使曝光不充分的图像黑的更黑,白的更白. 如果图像的大多数像素灰度值分布在区间],[b a ,则可以使用图5.1(b)所示的映射函数: ??? ????><≤≤+---='b z z a z z b z a z a z a b z z z k k 1 11 )( (5.2) 若要突出图像中具有某些灰度值物体的细节,而又不牺牲其它灰度上的细节,可以采用分段灰度变换,使需要的细节灰度值区间得到拉伸,不需要的细节得到压缩,以增强对比度,如图5.1(c)所示.当然也可以采用连续平滑函数进行灰度变换,见图5.1(d). 这一方法存在的问题是,当直方图被延伸后,所得到的新直方图并不均匀,也就是说,各灰度值所对应的像素数并不相等.因此,更好的方法应该是既能扩展直方图,又能使直方图真正地呈现均匀性.
图像预处理方法
预处理就是在图像分析中,对输入图像进行特征抽取等前所进行的处理。输入图像 由于图像采集环境的不同,如光照明暗程度以及设备性能的优劣等,往往存在有噪声, 对比度不够等缺点。另外,距离远近,焦距大小等又使得人脸在整幅图像中间的大小和 位置不确定。为了保证人脸图像中人脸大小,位置以及人脸图像质量的一致性,必须对 图像进行预处理。图像预处理的主要目的是消除图像中无关的信息,滤除干扰、噪声, 恢复有用的真实信息,增强有关信息的可检测性和最大限度地简化数据,从而改进特征 抽取的可靠性? 人脸图像的预处理主要包括人脸扶正,人脸图像的增强,以及归一化等工作。人脸 扶正是为了得到人脸位置端正的人脸图像;图像增强是为了改善人脸图像的质量,不仅 在视觉上更加清晰图像,而且使图像更利于计算机的处理与识别。归一化工作的目标是 取得尺寸一致,灰度取值范围相同的标准化人脸图像 ⑷。 2.1几何规范化 由于图像在提取过程中易受到光照、 表情、姿态等扰动的影响,因此在识别之前需要 对图像做归一化的预处理⑷,通常以眼睛坐标为基准点,通过平移、旋转、缩放等几何仿射 变换对人脸图像进行归一化。因为人脸虽然是柔性的三维曲面,同一人脸因表情变化会有 差异,但相对而言人的两眼之间的距离变化不会很大,因此双眼的位置及眼距,就成为人脸 图像归一化的依据。 定位眼睛到预定坐标,将图像缩放至固定大小。通过平移、旋转、缩放等几何仿射变 换,可以对人脸图像做几何规范化处理,仿射变换的表达式为: 其中(u,v)表示输入图像中像素的坐标(x,y)表示输出图像中像素的坐标。将上式展开 可得 x a^u a ?1v a 31 y a^u a ?2v a 32 平移变换就是给图像中的所有点的坐标都加上 u 和v ,其变换表达式为 a ii a 12 0 [x,y,1] [u,v,1][a 2i a 31 a 22 0] a 32 1 (2-1) (2-2)
图像预处理方法
图像预处理方法 Company Document number:WTUT-WT88Y-W8BBGB-BWYTT-19998
预处理就是在图像分析中,对输入图像进行特征抽取等前所进行的处理。输入图像由于图像采集环境的不同,如光照明暗程度以及设备性能的优劣等,往往存在有噪声,对比度不够等缺点。另外,距离远近,焦距大小等又使得人脸在整幅图像中间的大小和位置不确定。为了保证人脸图像中人脸大小,位置以及人脸图像质量的一致性,必须对图像进行预处理。图像预处理的主要目的是消除图像中无关的信息,滤除干扰、噪声,恢复有用的真实信息,增强有关信息的可检测性和最大限度地简化数据,从而改进特征抽取的可靠性. 人脸图像的预处理主要包括人脸扶正,人脸图像的增强,以及归一化等工作。人脸扶正是为了得到人脸位置端正的人脸图像;图像增强是为了改善人脸图像的质量,不仅在视觉上更加清晰图像,而且使图像更利于计算机的处理与识别。归一化工作的目标是取得尺寸一致,灰度取值范围相同的标准化人脸图像[4]。 几何规范化 由于图像在提取过程中易受到光照、表情、姿态等扰动的影响,因此在识别之前需要对图像做归一化的预处理[4],通常以眼睛坐标为基准点,通过平移、旋转、缩放等几何仿射变换对人脸图像进行归一化。因为人脸虽然是柔性的三维曲面,同一人脸因表情变化会有差异,但相对而言人的两眼之间的距离变化不会很大,因此双眼的位置及眼距,就成为人脸图像归一化的依据。 定位眼睛到预定坐标,将图像缩放至固定大小。通过平移、旋转、缩放等几何仿射变换,可以对人脸图像做几何规范化处理,仿射变换的表达式为: ]100][1,,[]1,,[323122 211211 a a a a a a v u y x = (2-1) 其中(u,v)表示输入图像中像素的坐标(x,y)表示输出图像中像素的坐标。将上式展开可得 32221231 2111u a x a v a u a y a v a ++=++= (2-2) 平移变换就是给图像中的所有点的坐标都加上u ?和v ? ,其变换表达式为 ]1 u 0100 01][1,,[]1,,[v v u y x ??= (2-3) 将图像中的所有点相对于坐标原点逆时针旋转θ角的变换表达式为 ]1 000cos sin 0sin cos ][1,,[]1,,[θθ θθ -=v u y x (2-4) 缩放变换既是将图像按给定的比例r 放大或缩小,当1>r 时图像被放大,当10< 图像预处理流程: 图2.2 图像预处理流程图 2.2 系统功能的实现方法 系统功能的实现主要依靠图像处理技术,按照上面的流程一一实现,每一部分的具体步骤如下: 1原始图像:由数码相机或其它扫描装置拍摄到的图像; 2预处理:对采集到的图像进行灰度化、图像增强,滤波、二值化等处理以克服图像干扰; 3字轮定位:用图像剪切的方法获取仪表字轮; 4字符分割:利用字符轮廓凹凸检测定位分割方法得到单个的字符; 5字符识别:利用模板匹配的方法与数据库中的字符进行匹配从而确认出字符,得到最后的仪表示数。 2.3.1 MATLAB简介 MATLAB 是美国MathWorks公司出品的商业数学软件,用于算法开发、数据可视化、数据分析以及数值计算的高级技术计算语言和交互式环境,主要包括MATLAB和Simulink两大部分。 MATLAB是矩阵实验室(Matrix Laboratory)的简称,和Mathematica、Maple并称为三大数学软件。它在数学类科技应用软件中在数值计算方面首屈一指。MATLAB可以进行矩阵运算、绘制函数和数据、实现算法、创建用户界面、连接其他编程语言的程序等,主要应用于工程计算、控制设计、信号处理与通讯、图像处理、信号检测、金融建模设计与分析等领域。 MATLAB的基本数据单位是矩阵,它的指令表达式与数学、工程中常用的形式十分相似,故用MATLAB来解算问题要比用C,FORTRAN等语言完相同的事情简捷得多,并且mathwork也吸收了像Maple等软件的优点,使MATLAB成为一个强大的数学软件。在新的版本中也加入了对C,FORTRAN,C++ ,JAVA的支持。可以直接调用,用户也可以将自己编写的实用程序导入到MATLAB函数库中方便自己以后调用,此外许多的MATLAB爱好者都编写了一些经典的程序,用户可以直接进行下载就可以用。 2.3.2 MATLAB的优势和特点 1、MATLAB的优势 (1)友好的工作平台和编程环境 MATLAB由一系列工具组成。这些工具方便用户使用MATLAB的函数和文件,其中许多工具采用的是图形用户界面。包括MATLAB桌面和命令窗口、历史命令窗口、编辑器和调试器、路径搜索和用于用户浏览帮助、工作空间、文件的浏览器。随着MATLAB的商业化以及软件本身的不断升级,MATLAB 的用户界面也越来越精致,更加接近Windows的标准界面,人机交互性更强,操作更简单。而且新版本的MATLAB提供了完整的联机查询、帮助系统,极大的方便了用户的使用。简单的编程环境提供了比较完备的调试系统,程序不必经过编译就可以直接运行,而且能够及时地报告出现的错误及进行出错原因分析。 《计算机视觉技术》作业 图像预处理综述 在图像信息输入系统获取原图像的过程中,由于所通过的传输介质的实际性能和接收设备性能的限制,不可避免地存在着外部干扰和内部干扰,因此所获得的图像通常都含有各种各样的噪声和畸变,大大影响了图像的质量。因此,在对图像进行分析之前,必须先对图像质量进行改善,通常采用图像增强的方法。 图像增强作为一种预处理技术,能使处理后的图像比原图像更适合于参数估计、图像分割和目标识别等后续图像分析工作。它不会考虑引起图像质量下降的原因,而是将图像中感兴趣的特征有选择的突出,并衰减不需要的特征。其主要目的有两个:一是改善图像的视觉效果,去除噪音,提高图像成分的清晰度;二是使图像变得更有利于计算机处理。因此,图像增强技术的研究是图像处理、计算机视觉和模式识别中的一项重要内容。 图像增强的方法一般分为空间域和变换域两大类。空间域方法通常都是先求取图像的灰度直方图,对灰度直方图处理后,求得映射函数,将原图像进行灰度映射。该类方法适用于对灰度级动态范围的控制,计算量较小,其中常用的是直方图均衡方法(HE)和平台直方图均衡方法(PE),具有一定的自适应性;而变换域方法是在图像的某个变换域中对变换系数进行处理,然后通过逆变换获得增强图像。直方图均衡化算法和降噪滤波法是图像增强空间域法中最常用的算法。 1 直方图均衡化算法 图像直方图均衡化是图像预处理中一种十分重要的分析工具,它能够反映数字图像的概貌性描述。例如:图像的灰度范围,灰度的分布,整幅图像的平均亮度和阴暗对比度等。直方图均衡化也叫直方图均匀化,就是把给定图像的直方图分布改变成均匀分布的直方图,它是一种比较常用的灰度增强算法。直方图有以下特点: 1) 直方图是一幅图像中各像素灰度出现频次的统计结果,它只反映图像中不同灰度值出现的次数,而不反映某一灰度所在的位置。 2) 任何一幅图像,都有惟一确定的与它对应的直方图,但不同的图像可能有相同的直方图。 3) 由于直方图是对具有相同灰度值的像素统计得到的,因此,一幅图像各子区的直方图之和就等于该图像全图的直方图。 直方图均衡化是把原始图像的直方图变换成均匀分布的形式,是以累计变换函数分布为基础的,从而产生一幅灰度级分布具有均匀概率密度的图像。它以概率理论作基础,运用灰度点运算来实现直方图的变换,从而达到图像增强的目的。 直方图均衡化算法如下: (1) 计算原始图像的所有灰度级k s ,0,1, ,1k L =-; (2) 统计原始图像各灰度级的像素数k n ; (3) 计算原始图像的直方图: ()()0,1,,1k k p k L n n s ==- (4) 计算原始图像的累计直方图: 第五章 一个带通滤波通过从相应的带阻滤波而获得: 然后: (a )理想带通滤波: (b )巴特带通滤波: (c )高斯带通滤波: 带阻滤波器公式可以通过带通滤波器的公式得到。两者的和为 1. H n ,U,V) 1 H n p (U,V) 然后: (a) 理想带阻滤波: H(u,v), 其他 2.巴特带阻滤波: 我不想输这个公式了,这个就是下面的巴特带通滤波的公式中 1减的后面那个式子 (b) 巴特带通滤波: 3.高斯带阻滤波: 我不想输这个公式了,这个就是下面的高斯带通滤波的公式中 (c) 高斯带通滤波: D i (u,v) D °,或 D 2 ( u ,v ) D ° 1减的后面中括号那个式子 二维连续余弦函数的傅里叶变换 F(u,v) f (u,v)e j2 (ux vy)dxdy Acos(u0x v0y)e j2 (ux vy)dxdy 余弦的变换 1 cos (e i e J ) 2 带入得到 F(u,v) A [e J(Uox voy)e J(u°xvoy)]e J2(uxvy)dxdy A[ e J2 (u°x/2 v°y/2 )e J2 (ux vy)dxdy] A[ e J2 (u°x/2 v°y/2 )e J2 (ux vy)dxdy] 这些都是傅里叶变换的功能 并且 结果变换成 / u°v°u°v° F(u,v) [ (u -,v -) (u -,v -)]即可 2 2 2 2 2 从例子() 即因此 得出 这是一个持续的形式, 一个高斯密度方差 或者 减去的整体从无限数量的加上括号里面是1,因此 这个两个题的区别比较小,但是结果有区别,在书上没有找到吧两者 的答案都写上吧,英语的翻译版的估计大些, 解决这个问题的关键是要认识到下面给定的函数, 是的二阶导数(拉普拉斯算子)的功能(参见 3.6.2 节有关拉普拉斯算子) 即, 所以, 但是,我们知道 这里 因此,我们已经降低了计算的傅里叶变换的问题的高斯函数。从高斯傅立叶变换对的基本形式条目13的表中给出(附注(的x, 丫)和(u, v)的在本问题是反向的表中的条目), 所以我们有最终结果 这是一个简单的扩展的问题。其目的是为了熟悉维纳滤波的各种条 件, 第一章绪论 1.模拟图像处理与数字图像处理主要区别表现在哪些方面? (什么是图像?什么是数字图像?什么是灰度图像?模拟图像处理与数字图像处理主要区别表现在哪些方面?) 图像:是对客观对象的一种相似性的、生动性的描述或写真。 数字图像:一种空间坐标和灰度均不连续的、用离散数字(一般用整数)表示的图像。 灰度图像:在计算机领域中,灰度数字图像是每个像素只有一个采样颜色的图像。在数字图像领域之外,“黑白图像”也表示“灰度图像”,例 如灰度的照片通常叫做“黑白照片”。 模拟图像处理与数字图像处理主要区别:模拟图像处理是利用光学、照相方法对模拟图像的处理。(优点:速度快,一般为实时处理,理论上讲可达到光的速度,并可同时并行处理。缺点:精度较差,灵活性差,很难有判断能力和非线性处理能力) 数字图像处理(称计算机图像处理,指将图像信号转换成数字格式并利用计算机对数据进行处理的过程)是利用计算机对数字图像进行系列操作,从而达到某种预期目的的技术.(优点:精度高,内容丰富,可进行复杂的非线性处理,灵活的变通能力,一只要改变软件就可以改变处理内容) 2.图像处理学包括哪几个层次?各层次间有何区别和联系? 数字图像处理可分为三个层次:狭义图像处理、图像分析和图像理解。 狭义图像处理是对输入图像进行某种变换得到输出图像,是一种图像到图像的过程。 图像分析主要是对图像中感兴趣的目标进行检测和测量,从而建立对图像目标的描述,图像分析是一个从图像到数值或符号的过程。 图像理解则是在图像分析的基础上,基于人工智能和认知理论研究图像中各目标的性质和它们之间的相互联系,对图像内容的含义加以理解以及对原来客观场景加以解译,从而指导和规划行动。 区别和联系:狭义图像处理是低层操作,它主要在图像像素级上进行处理,处理的数据量非常大;图像分析则进入了中层,经分割和特征提取,把原来以像素构成的图像转变成比较简洁的、非图像形式的描述;图像理解是高层操作,它是对描述中抽象出来的符号进行推理,其处理过程和方法与人类的思维推理有许多类似之处。 3.图像处理与计算机图形学的区别与联系是什么? 数字图像处理,是指有计算机及其它有关的数字技术,对图像施加某种运算和处理,从而达到某种预期的目的,而计算机图形学是研究采用计算机生成,处理和显示图形的一门科学。 二者区别:研究对象不同,计算机图形学研究的研究对象是能在人的视觉系统中产生视觉印象的事物,包括自然景物,拍摄的图片,用数学方法描述的图形等,而数字图像处理研究对象是图像;研究内容不同,计算机图像学研究内容为图像生成,透视,消阴等,而数字图像处理研究内容为图像处理,图像分割,图像透 2.2系统功能的实现方法 系统功能的实现主要依靠图像处理技术,按照上面的流程一一实现,每一部分的具体步骤如下: 1原始图像:由数码相机或其它扫描装置拍摄到的图像; 2预处理:对采集到的图像进行灰度化、图像增强,滤波、二值化等处理以克服图像干扰; 3字轮定位:用图像剪切的方法获取仪表字轮; 4字符分割:利用字符轮廓凹凸检测定位分割方法得到单个的字符; 5字符识别:利用模板匹配的方法与数据库中的字符进行匹配从而确认出字符,得到最后的仪表示数。 2.3.1MATLA B简介 MATLAB是美国MathWorks公司出品的商业数学软件,用于算法开发、数据可视化、数据分析以及数值计算的高级技术计算语言和交互式环境,主要包括MATLAB和Simulink 两大部分。 MATLAB是矩阵实验室(MatrixLaboratory)的简称,和Mathematica、Maple并称为三大数学软件。它在数学类科技应用软件中在数值计算方面首屈一指。MATLAB可以进行矩阵运算、绘制函数和数据、实现算法、创建用户界面、连接其他编程语言的程序等,主要应用于工程计算、控制设计、信号处理与通讯、图像处理、信号检测、金融建模设计与分析等领域。 MATLAB的基本数据单位是矩阵,它的指令表达式与数学、工程中常用的形式十分相似,故用MATLAB来解算问题要比用C,FORTRAN等语言完相同的事情简捷得多,并且mathwork也吸收了像Maple等软件的优点,使MATLAB成为一个强大的数学软件。在新的版本中也加入了对C,FORTRAN,C++,JAVA的支持。可以直接调用,用户也可以将自己编写的实用程序导入到MATLAB函数库中方便自己以后调用,此外许多的MATLAB爱好者都编写了一些经典的程序,用户可以直接进行下载就可以用。 2.3.2MATLAB的优势和特点 1、MATLAB的优势 (1)友好的工作平台和编程环境 图像增强GUI的fig界面 图像增强GUI的结果界面 其m文件见txt文件: 图像增强GUI的m文件: function varargout = imageenhance(varargin) % IMAGEENHANCE MATLAB code for imageenhance.fig % IMAGEENHANCE, by itself, creates a new IMAGEENHANCE or raises the existing % singleton*. % % H = IMAGEENHANCE returns the handle to a new IMAGEENHANCE or the handle to % the existing singleton*. % IMAGEENHANCE('CALLBACK',hObject,eventData,handles,...) calls the local % function named CALLBACK in IMAGEENHANCE.M with the given input arguments. % % IMAGEENHANCE('Property','V alue',...) creates a new IMAGEENHANCE or raises the % existing singleton*. Starting from the left, property value pairs are % applied to the GUI before imageenhance_OpeningFcn gets called. An % unrecognized property name or invalid value makes property application % stop. All inputs are passed to imageenhance_OpeningFcn via varargin. % % *See GUI Options on GUIDE's Tools menu. Choose "GUI allows only one % instance to run (singleton)". % % See also: GUIDE, GUIDATA, GUIHANDLES % Edit the above text to modify the response to help imageenhance % Last Modified by GUIDE v2.5 19-May-2012 20:00:36 % Begin initialization code - DO NOT EDIT gui_Singleton = 1; gui_State = struct('gui_Name', mfilename, ... 'gui_Singleton', gui_Singleton, ... 'gui_OpeningFcn', @imageenhance_OpeningFcn, ... 'gui_OutputFcn', @imageenhance_OutputFcn, ... 'gui_LayoutFcn', [] , ... 'gui_Callback', []); if nargin && ischar(varargin{1}) gui_State.gui_Callback = str2func(varargin{1}); end if nargout [varargout{1:nargout}] = gui_mainfcn(gui_State, varargin{:}); else gui_mainfcn(gui_State, varargin{:}); end % End initialization code - DO NOT EDIT图像预处理流程
图像预处理综述
数字图像处理第三版第五章答案
图像处理课后习题
图像预处理操作规范
图像预处理GUI